


BS”D
French whistleblower calculations demonstrate the existence of a very significant increase in the number of deaths of babies aged two to six days, two months in a row, exactly since the introduction of this “preventive monoclonal therapy against bronchiolitis” (Beyfortus®) in France.
Last summer and fall, we watched in grave concern as the RSV shots were approved. We worried about newborns being given the shots at birth without their parents’ understanding what they’re about, and I published articles at that time in an effort to raise the alarm.
Sadly, the RSV shots have gone into babies’ arms, sometimes with the tragically expected consequences. It’s my hope that by speaking out again, G-d willing, I will reach some additional people and save children.
(For clarity, there are three new RSV shots: a Pfizer vaccine for pregnant women and seniors, a GSK vaccine for seniors, and an Astra Zeneca – Sanofi monoclonal antibody shot for babies. They are all terrible news. In this article, I am focusing mostly on the newborn shots.)
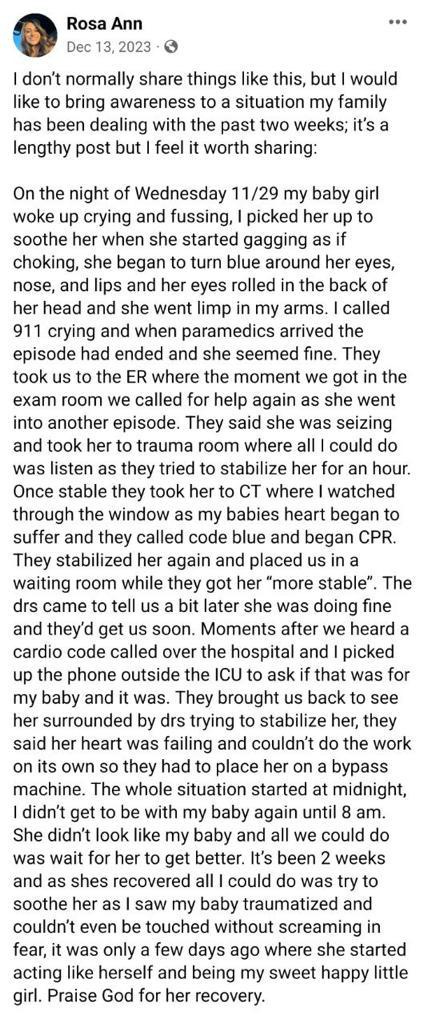
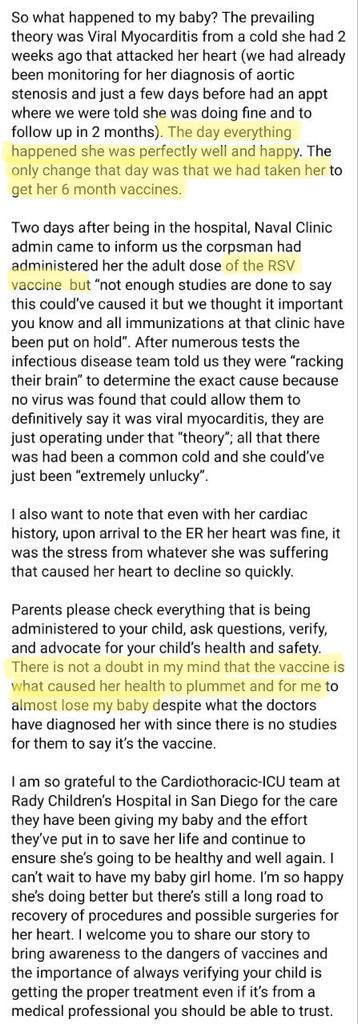
Here is a very fortunate baby who almost didn’t make it – but thank G-d survived the cardiac adverse effects of the RSV shot:
Here is part of Sasha Latypova’s January article detailing the horror happening in France with the mass administration to newborns of RSV monoclonal antibodies and the concurrent spike in newborn deaths.
Protect Babies from the Injection of Beyfortus (RSV monoclonal)
By Sasha Latypova
Helene Banoun is a pharmacist-biologist, former INSERM researcher, based in France.
She writes in an email:
Since December 6, when I alerted the public about the French government’s uncontrolled clinical trial, Twitter France has made me invisible. In France, the injection of Beyfortus (nirsevimab, a monoclonal antibody against bronchiolitis caused by RSV) is recommended for all newborns from the maternity ward. This treatment has not been tested on newborns, but on children aged between 3 months and 2 years!
French whistleblower calculations demonstrate the existence of a very significant increase in the number of deaths of babies aged two to six days, two months in a row, exactly since the introduction of this “preventive monoclonal therapy against bronchiolitis” (Beyfortus®) which has never really been tested in newborns.
It seems that Twitter has activated the “hide Hélène Banoun’s tweets” feature for many subscribers https://twitter.com/BanounHelene
“The unpleasant surprises of RSV bronchiolitis vaccines and preventive therapies.”
by Helene on Researchgate here.
Some excerpts from the paper [numbered references are in the linked paper]:
Monoclonal antibody preventive therapies?
A new concept is emerging in the fight against bronchiolitis: preventive therapy involving direct injection of antibodies. In collaboration with Astra-Zeneca, Sanofi is marketing a monoclonal antibody against RSV, Beyfortus, for preventive injections in newborns. One of the clinical trials [1] showed serious adverse reactions to the vaccine, with 3 deaths in the vaccinated group versus 0 in the placebo group. According to the ritual formula, “deaths are not attributed to the vaccine by the investigator”.
The FDA recorded 12 deaths in all trials of this monoclonal antibody [2]: 4 cardiac deaths, 2 gastroenteritis, 2 sudden deaths, 1 cancer, 1 Covid, 1 fracture, 1 pneumonia, but no deaths were linked to treatment.
The EMA recorded 3 deaths in the placebo groups and 11 deaths in the treatment groups. EMA conclusion: the benefit/risk balance is positive…[3].
The HAS (Haute Autorité de Santé, High Health Authority, France) also stresses the absence of any data to support a possible impact on reducing hospitalization times or mortality, and also notes deaths as a possible adverse effect [4].
Let’s not forget that this whole bronchiolitis “prevention” campaign is supposed to avoid overcrowding hospitals with babies suffering from this disease: if this product doesn’t significantly reduce hospitalizations, what’s the point?
In its September 2022 report [3], the EMA reminds us of the fiasco of RSV vaccine trials in the past: children died of severe bronchiolitis in the vaccinated groups and none in the control groups.
This is yet another manifestation of the ADE (antibody-mediated facilitation/aggravation of infection) described for Dengue fever [5]. This ADE is due to the deleterious effect of antibodies which, instead of neutralizing the virus, facilitate its entry into the cell via the receptor of the Fc fragment of immunoglobulins.
And it’s precisely this Fc region of Nirsevimab (the generic name for Beyfortus) that industry has seen fit to modify: the Fc of this antibody has a higher affinity for the neonatal Fc receptor, in order to extend its lifespan.
The EMA reminds us that the role of this Fc fragment in “protection” against the RSV virus cannot be ruled out. As I explained [6], different names are given to the same phenomenon, depending on whether it’s considered beneficial (ADCD, ADNKA, ADCP, ADNP) or deleterious (ADE): it’s always an entry of the virus into the cell facilitated by the Fc fragment of the antibody. Manufacturers are looking for the beneficial effects of this phenomenon and are wary of deleterious effects, which is why they have investigated the risk of ADE with Beyfortus in animal models. They claim not to have detected it, but the EMA points out, unmoved, that no histopathological evaluation of rats was carried out after treatment and infection with RSV: this is the only recognized marker of ADE.
The EMA reassures us that no signs of ADE have been observed in clinical trials: really? However, bronchiolitis was reported as the cause of death in infants in the treated groups; these deaths were not attributed to the treatment by the investigator. To be able to confirm this, these poor babies would have had to be autopsied and checked for histopathological phenomena in the lungs: this was not done, and the EMA was careful not to ask for it. It is therefore to be feared that this monoclonal antibody, whose Fc fragment has been modified, could cause this dangerous ADE effect in certain infants, which would explain the imbalance in deaths in the treated group compared to placebo, but also the same imbalance compared to the group treated with Synagis (palivizumab), the former equivalent drug which did not have this modification of the Fc fragment [7]!
BW: See below for the firsthand story of a tragic baby death resulting from the Palivizumab RSV monoclonal, as related to me by the child’s mother. I find the information provided by Helene Banoun very enlightening, as until now I had not been aware that monoclonals could also potentially cause ADE. The Palivizumab death below (claimed to be “from RSV” – and immediately after receiving the monoclonal shot) makes even more sense now.
An article in French press (auto translation to English available) “The Beyfortus train has already derailed.” Shows the following grim statistics:
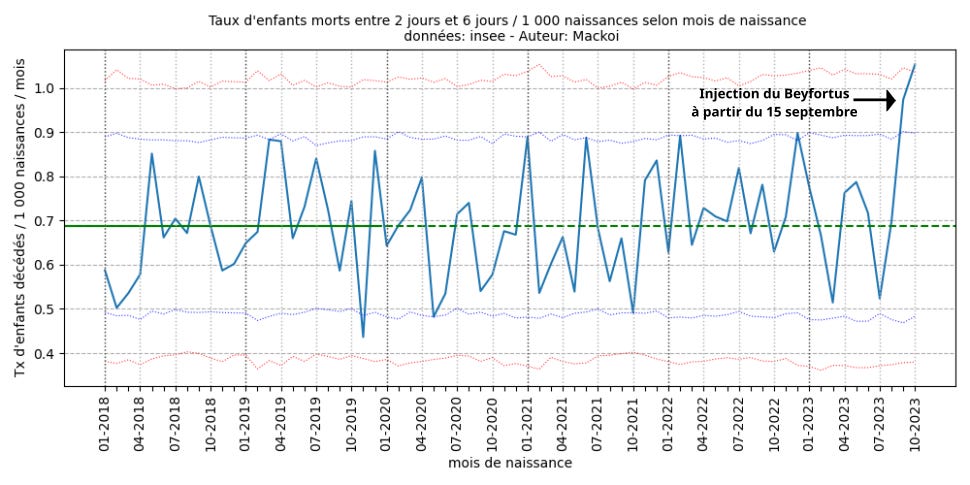
The blue curve represents, for each month (from 2018 to October 2023), the mortality rates of 2 to 6 days of life, of the native babies of the month in question.
- The horizontal green line represents the reference rate, calculated over the years 2018-2019. This rate is 0.69 deaths per 1,000 births.
- The blue dotted lines represent the’ confidence interval of the mortality rates at 95 %.
- The red dotted lines represent the’ confidence interval of the mortality rates at 99.8 %.
As of September 2023, there are 54 infant deaths between 2 and 6 days of life out of 55,489 births, what gives a mortality rate of 0.97 deaths per 1,000 births.
White House Confirms 230,000 Additional RSV Immunization Doses for Infants Next Month.
(End of quotes.) See Sasha’s entire January 6 article on her substack, SashaLatypova.substack.com.
It is horrifying that health officials want to routinely give the new monoclonal antibody, nirsevimab, to newborns on their first day of life.
Never before were monoclonals given to babies – except the sickest ones, or given to any segment of the population on a mass scale. Anaphylactic reactions are absolutely expected to happen in a percentage of recipients. What are headed for? THIS IS INSANE!
I received from a subscriber in Israel a heartbreaking story of loss of a then-only child, directly resulting from the previously used RSV monoclonal antibody shot, which was given to high risk babies – Palivizumab (Abbosynagis/Synagis.) I’m going to copy her emails and documents here:
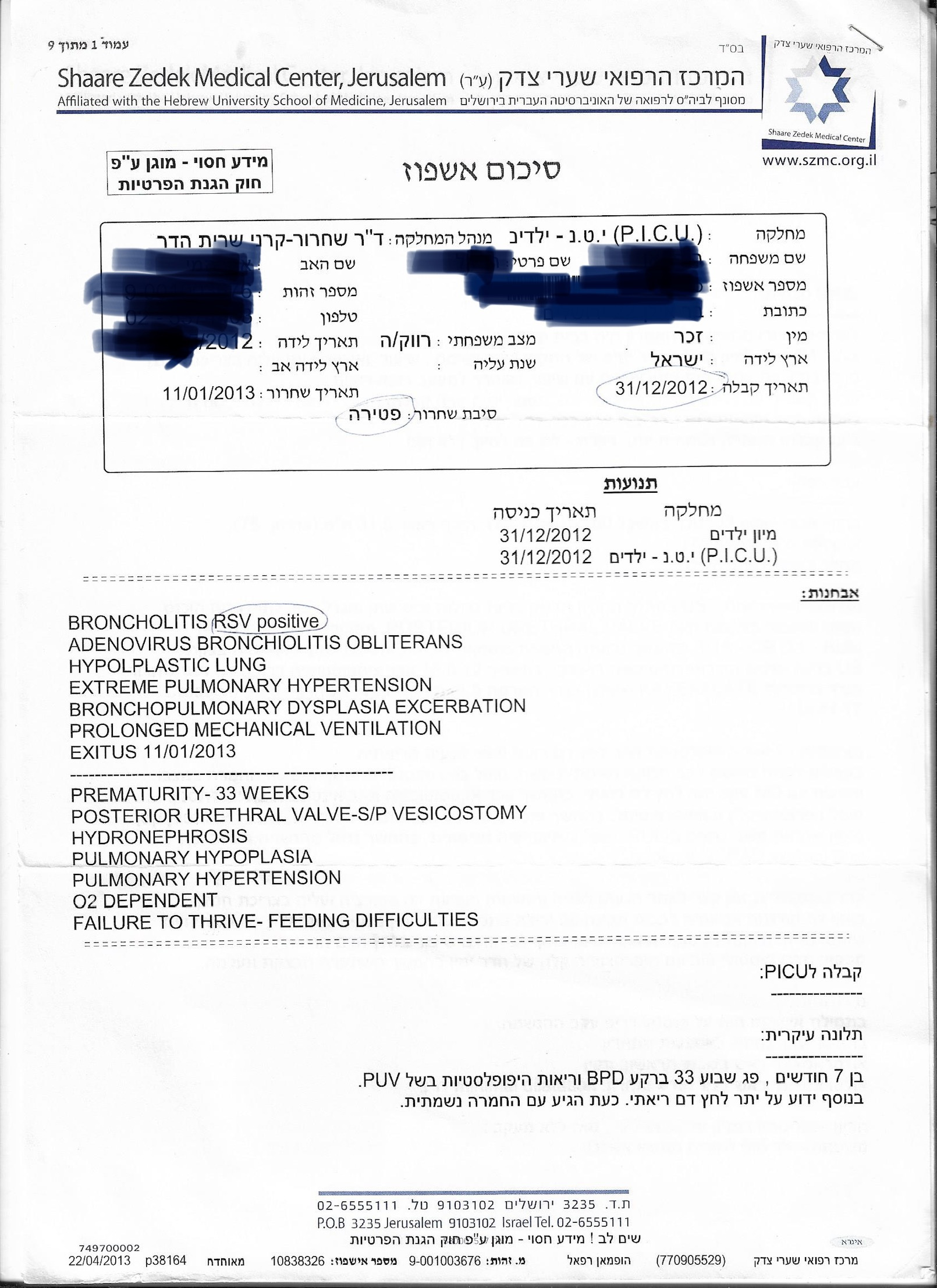
“My 8-month old baby passed away from an RSV shot!!!! (January 2013) Nobody believes me but you will! He was given his third (monthly) shot. In the clinic he stopped breathing.
I took him to hospital immediately where a culture confirmed he has RSV in his system. He was intubated 3 days later, and passed away 12 days after the shot, from RSV.
I have proof on his death certificate: Reason of death: RSV infection.”
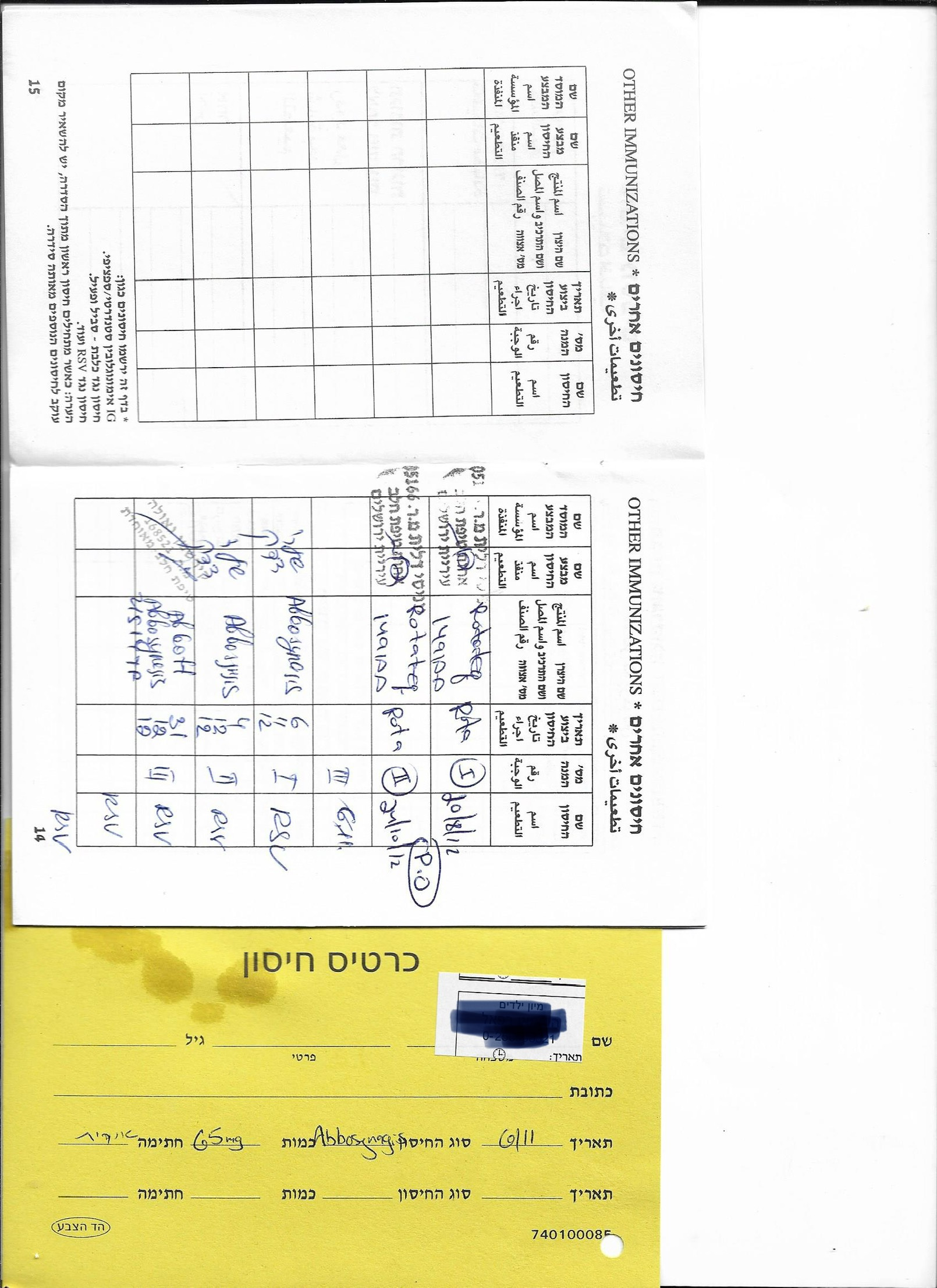
“Note the last time he received it was 31/12/12, and the last time he was admitted to hospital was on the same day! (Immediately after…. but they omitted this very crucial info….)
I hope this is enough to persuade parents to not let their child go under the knife of the Angel of Death.”
RSV shots have until now been the epitome of a failed vaccine, with a negative efficacy (the shots made things worse when people were exposed to the illness), causing ADE and death in trials. There is not enough reason to believe things will now be rosy.
What is ADE? This article from CHOP explains the basic idea, while also being very obfuscating and tricky (how would “breakthrough disease” be distinguished from ADE?)

See these articles explaining how the original RSV shots caused worsened disease and death, and how unsure scientists are about the new “fix:”

Almost 80 percent of the children who were vaccinated for RSV in the 1960’s trial and then exposed to RSV, were hospitalized for severe illness! Two toddlers died. In other words, the vaccine did exactly the opposite of what it was supposed to do. It made everything much worse.
Further from the Tulane site:
“The cause of these toddlers’ deaths was a medical mystery for decades — until now, according to a new study co-authored by Tulane University researchers in the journal Science Translational Medicine.
“After encountering RSV infection, the toddlers from the 1960s developed lung injury that damaged critical lung cells, said study co-corresponding author Dr. Jay Kolls, John W Deming Endowed Chair in Internal Medicine at Tulane School of Medicine.
“These two children died likely due to injury to surfactant producing cells in the lung that are critical for transporting oxygen to the blood,” Kolls said. “Our study provides a comprehensive characterization of fatal enhanced respiratory disease, a tragedy that hampered RSV vaccine development for decades.”
The conclusion on Tulane’s page: “The results of the study could make future attempts at developing an RSV vaccine safer by providing a molecular signature of enhanced RSV disease. Future vaccine developers can look for these markers when they test promising candidates in preclinical models.
“They can look for the same gene signatures that we identified,” Kolls said. “If they can show that their vaccine doesn’t elicit any of that kind of response, I think that would give both a potential funding sponsor or the FDA some comfort level that the vaccine is safe.” (Most emphases mine.)
“Some comfort level that the vaccine is safe.” (?!!) How is some comfort level good enough, when playing with lives?
Look how little a key scientist involved in the RSV vaccine development, Barney Graham, actually understands about antibody dependent enhancement (ADE.) This is from his November 2022 interview with Science.
“The enhancement is a complicated story and we think we understand parts of it. It’s like looking through a mirror darkly type of understanding.”
Graham has huge financial conflicts of interest: the Science article reports that “Graham has a patent on the RSV F design and stands to receive royalties if the vaccine reached the market. After leaving NIAID last year, he also began consulting with Pfizer and several other vaccine companies.”
Indeed, Barney Graham worked under Anthony Fauci at the NIAID beginning in 2000, and stands to personally earn $150,000 yearly in royalties on the new RSV vaccine.
Greed for profit certainly explains a lot, but not everything.
It is particularly disturbing to me that this monoclonal “vaccine” for newborns is coming from AstraZeneca, a company with known ties to the eugenics movement.
See the December 2020 investigative article below.
The authors found it highly suspect that the AstraZeneca covid vaccine was being deployed to the same areas of the world whose populations the eugenicists have expressed their desire to diminish.
I feel the similarly at present, regarding AstraZeneca’s baby RSV shot, especially considering the curiosity of how “generously” it is being made available to Native American and Alaskan Native older babies. Eugenicists have a long history of seeking to decimate native populations.
Here is a screenshot of some relevant parts of the lengthy article.

(Note, my citation of this article does NOT imply my agreement with any other content the authors may have on their site.)
Link to article:
Parents, JUST SAY NO!
Your baby’s chances of coming to grave harm from the RSV shots are much greater than his or her chances of coming to grave harm from the RSV illness itself.
